

A recent publication in JBJS has called attention to an important topic in shoulder instability: glenoid bone loss. Glenoid loss directly influences the mechanism of concavity-compression, which has previously been discussed. Loss of glenoid width, due to loss of the glenoid rim, will result in a significant challenge to maintain the humeral head on the glenoid face.

Loss of bone can occur either suddenly (from a fracture), or over time due to attritional loss of bone from repeated episodes of instability. Multiple dislocations can lead to erosion of the rim – hence we commonly recommend surgery for first time dislocators, partly anticipating that stabilization could potentially prevent loss of bone (although this concept has not been validated).
What is the threshold of loss?
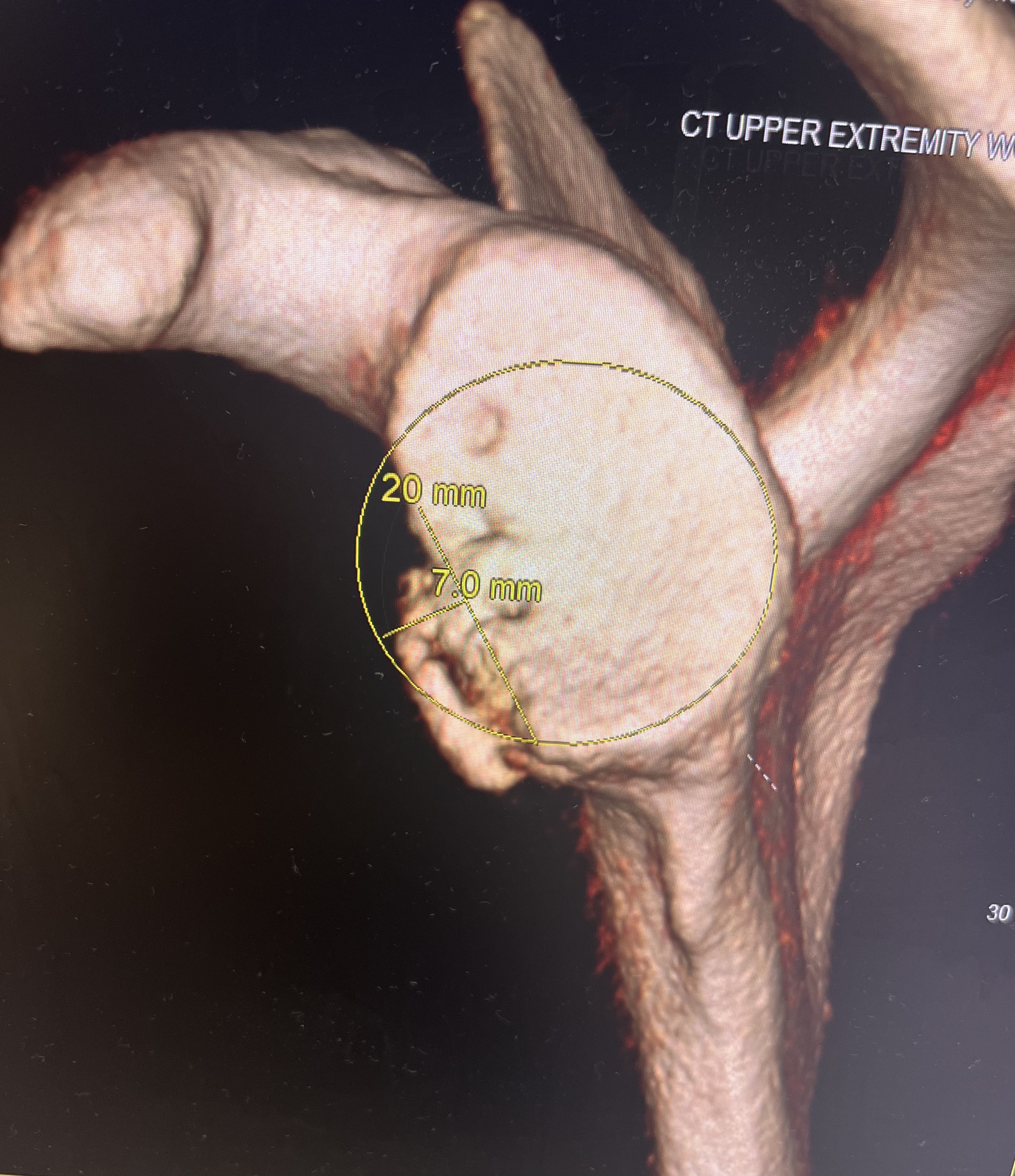
The normal glenoid should fill a circle on the bottom 2/3 of the glenoid. It is generally accepted that loss of 20-25% of the glenoid width requires some sort of bone reconstruction to restore the glenoid concavity. Soft tissue repairs have proven unsuccessful with larger defects. Burkhart first identified the “inverted pear” glenoid and the impact of bone loss on outcomes of stabilization1. Since then, numerous studies have correlated failure of Bankart repair to loss of bone.

The glenoid track, initially described by Yamamoto in 20072, accounts for combined defects of the glenoid and humeral head (Hill Sacs lesion). These combined defects are immensely important to identify and address, and looking at glenoid loss in isolation is likely not helpful as we determine how best to stabilize the shoulder. Concavity-compression requires both a full convex surface and a wide concave surface that can be compressed together.
Different treatment algorithms have been developed that describe optimal surgical intervention based on amount of bone loss. Arthroscopic bankart repair, open Bankart, +/- remplissage, coracoid transfer (Latarjet and its modifications and technique variations), and free bone graft (distal tibia, iliac crest, and distal clavicle) have been employed in the management of glenoid bone loss. These pathways have been developed based on literature as well as surgeon experience and training. An excellent summary was provided in 2017, complete with references for further reading3.
Open vs Arthroscopic Repair
While at the University of Washington in 2004, I helped author a meta-analysis comparing these approaches for restoring stability to the unstable traumatic anterior dislocator4. We showed that open repairs were a bit more reliable than the arthroscopic techniques being used at that time (arthroscopic techniques were impaired by lack of use of remplissage, and an inability to get low on the glenoid). However, arthroscopic techniques seemed to provide better functional scores for patients. Better function came at the risk of worse stability. Tightening one shoulder more than another may lead to better stability, but worse function. Achieving both stability and mobility may be difficult to achieve for the operative surgeon using the various surgical techniques.

This finding, along with improved technology and available devices for repair, has helped drive a push toward utilization of arthroscopic repairs. Open Bankart has become a forgotten procedure, as many recent graduates of Orthopedic Surgery training programs may have never seen an open Bankart repair.
We have recently looked at outcomes of our open Bankart repair using a modification of the technique described by Thomas and Matsen in their 1989 publication (which showed only 5% rate of recurrence)5. In unpublished data, we found very low recurrent rates of instability in 50 patients with glenoid and humeral deficiency (“off track” lesions). Zero of the 9 patients with off track lesions experienced recurrent instability. However, 6% of our study population experienced failure of the stabilization, and another 6% didn’t trust their shoulder. All of these failures had a prior stabilization procedure. Short term follow-up has prevented publication of this data. Open Bankart is reliable, but maybe less so in the revision setting.
What does this new publication by Min tell us?
This new systematic review by Min, et al., looked at relatively low quality level of evidence and summarized that a 16% loss of glenoid width places one at risk of failure with arthroscopic stabilization. Additionally, a loss of 20% glenoid width predicted worse clinical outcomes even in the absence of recurrent instability.
The paper was not able to evaluate the influence of remplissage on recurrence rates. They also did not compare arthroscopic repair to open repair or bone reconstructive procedures.
It seems that predictable outcomes for arthroscopic repair can be achieved with minimal glenoid loss, few episodes of instability, non contact sports participation. However, if these conditions exist, then the scope is likely not the best choice for our patients.
What next?
A trend toward use of remplissage with arthroscopic repair may improve outcomes. Studies suggest lower rates of recurrence with remplissage6. Simple techniques are available, that are relatively easy to learn and perform. Technology has driven this learning curve.
We should not forget about the open Bankart, especially the technique described by Thomas and Matsen. It is a reliable procedure, even in the presence of bone loss. There may be advantages of open Bankart compared to bone reconstruction – it more “anatomic”, avoids the need to harvest the coracoid or allograft tissue, and can be reliably taught and executed. Open Bankart is one of my own favorite procedures to perform. A predictable, routine procedure that can be offered to patients who are struggling to achieve a stable shoulder. Limits exist, of course. I still lean on 20-25% loss as a criteria for use of Latarjet or Distal Tibia allograft.
What we need are studies comparing a well done open Bankart and arthroscopic Bankart + remplissage. Level I data to guide our decision and strengthen our treatment algorithms. For now – I’ll continue to use what I know works best in my hands. OPEN BANKART is the way!
References
- Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000 Oct;16(7):677-94. doi: 10.1053/jars.2000.17715. PMID: 11027751. ↩︎
- Yamamoto N, Itoi E, Abe H, Minagawa H, Seki N, Shimada Y, Okada K. Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: a new concept of glenoid track. J Shoulder Elbow Surg. 2007 Sep-Oct;16(5):649-56. doi: 10.1016/j.jse.2006.12.012. Epub 2007 Jul 23. PMID: 17644006. ↩︎
- Rabinowitz J, Friedman R, Eichinger JK. Management of Glenoid Bone Loss with Anterior Shoulder Instability: Indications and Outcomes. Curr Rev Musculoskelet Med. 2017 Dec;10(4):452-462. doi: 10.1007/s12178-017-9439-y. PMID: 28994027; PMCID: PMC5685961. ↩︎
- Lenters TR, Franta AK, Wolf FM, Leopold SS, Matsen FA 3rd. Arthroscopic compared with open repairs for recurrent anterior shoulder instability. A systematic review and meta-analysis of the literature. J Bone Joint Surg Am. 2007 Feb;89(2):244-54. doi: 10.2106/JBJS.E.01139. PMID: 17272436. ↩︎
- Thomas SC, Matsen FA 3rd. An approach to the repair of avulsion of the glenohumeral ligaments in the management of traumatic anterior glenohumeral instability. J Bone Joint Surg Am. 1989 Apr;71(4):506-13. PMID: 2703510. ↩︎
- Davis WH, DiPasquale JA, Patel RK, Sandler AB, Scanaliato JP, Dunn JC, Parnes N. Arthroscopic Remplissage Combined With Bankart Repair Results in a Higher Rate of Return to Sport in Athletes Compared With Bankart Repair Alone or the Latarjet Procedure: A Systematic Review and Meta-analysis. Am J Sports Med. 2023 Oct;51(12):3304-3312. doi: 10.1177/03635465221138559. Epub 2023 Jan 9. PMID: 36622005. ↩︎
Leave a Reply