
“A high position of the humeral component relative to the greater tuberosity was the most common problem with humeral component positioning”
Franta, Lenters, Mounce, Neradilek, Matsen
“SAFE” study JSES 2007
Glenoid side
Shoulder surgeons have recognized the importance of glenoid component positioning in outcomes of anatomic shoulder arthroplasty. Many surgeons have bolstered their academic prowess by publishing data discussing version, Walch subtype, correction limits, and other factors relating to the glenoid. Despite extensive work on the glenoid side, we remain uncertain as to best surgical care for various subtypes, especially the B2 glenoid as it relates to patient demographics of age, activity level, bone quality, pre-operative ROM, and prior surgical care.
Humeral side
Less is known about the impact of humeral positioning on outcomes of anatomic replacement. I had an opportunity during my fellowship training at the University of Washington to investigate factors associated with dissatisfaction of the outcome of shoulder replacement. We determined that humeral component malposition is present in almost 2/3 of patients who are unhappy with their outcome.1 Although we didn’t show causation, it evident that a correlation between surgeon’s failure to properly position the humeral head and poor outcomes is predictably noted.


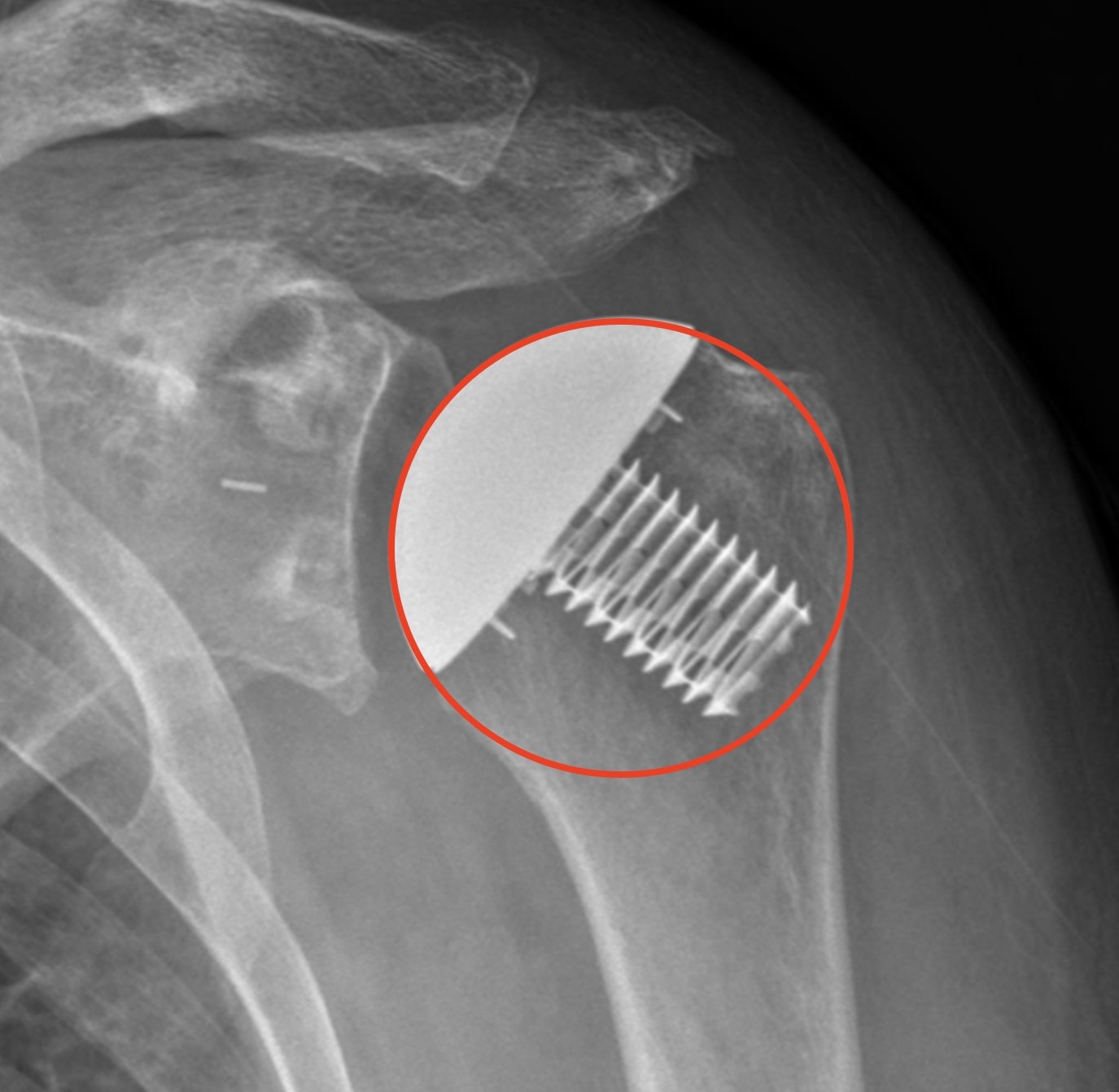
Historical papers didn’t necessarily recognize this issue, as seen in this image from a 2012 publication discussing failure of metal-back glenoids.2 The glenoid took the blame for this failed arthroplasty:

Important Humeral Metrics
We should discuss 2 separate, but related, factors involving the proximal humerus. One factor describes the position of the articular surface in relation the surrounding non-articular components of the humerus (the Iannotti circle3). Dr. Iannotti described a 3D sphere of the proximal humerus, which can be represented by a simple circle on a true Grashey AP view of the shoulder. Important markers of the circle include each end of the anatomic neck, and a point on the lateral aspect of the greater tuberosity. The native articular surface lies on this sphere, understanding some asymmetry of the head between the AP and the SI directions.

The second factor describes the center of rotation (COR) of the proximal humerus/humeral head. The COR is simply the center of the Iannotti circle.

The Iannotti circle and the COR are related, but separate factors. Changing one factor will likely have an impact on the other. However, one metric could be anatomically changed, leaving the other properly positioned. For example, moving the prosthetic COR away from native COR might appropriately position the humeral articular surface by changing the size of the head.

Likewise, moving the prosthetic humeral head off of the Iannotti circle might replicate the native COR by using an incorrect humeral head size.


Evidence
It seems plausible that replication of both the native COR and the Iannotti circle should be goals of surgical reconstruction. Of course, this is a soft tissue balancing procedure.I have been impressed that thorough releases/resection of contracted capsule, combined with restoration of native glenoid version and proper head size/position will almost universally lead to a well balanced and well functioning shoulder. If we release the soft tissues and correct the glenoid, the prosthetic humeral head should also be anatomic to give the most predictable outcome.
We have clear data relating overstuffing of the joint to rotator cuff failure, glenoid failure, pain, stiffness, and overall worse outcomes. But what is the threshold of the “stuff”? We can look to the existing literature for tolerances to change of the COR and Iannotti circle.
COR data
Brian Werner described in a 2021 JSES Seminars in Arthroplasty paper that a shift in COR of <2.7 mm led to better ROM and ASES scores when compared with shoulders that had a larger shift.4 The findings correlated with earlier biomechanical studies, which were cited in the study. These prior studies targeted anywhere from 2.5 mm to 5 mm as the threshold for optimum function of the replacement.
However, Chalmers could not find an association between a shift in COR and outcome of shoulder arthroplasty.5
The AAOS did not included a recommendation for COR shift in its Clinical Practice Guidelines (CPG) for shoulder arthoplasty.
Trying to summarize the data on COR is limited by the number of available clinical studies, but good practice would aim to keep the reconstructed COR within 2.5 mm of native COR.
Iannotti Circle data
Surprisingly, data discussing replication of the Iannotti circle is not available. Changing this metric is likely to have important influence on the outcome of shoulder replacement. With the advent of advanced planning and surgical techniques to assist with execution of these plans, thresholds for change can be developed. A safe assumption may be that the prosthetic humeral arc should lie within 2.5mm of the native Iannotti circle, but clinical data should corroborate this claim.
Next steps
Surgeons have a variety of means to influence their ability to achieve these appropriate metrics. The next post will discuss how the humeral cut, the selection of stemmed/stemless implants, virtual planning, and use of a guided neck cut impact surgical execution.
Summary
Replication of proximal humeral anatomy has important influence on outcome of anatomic shoulder arthoplasty. The COR and the Iannotti circle are 2 relevant metrics to utilize to achieve desired outcomes, and to avoid dissatisfaction with the outcome of the procedure. The COR should be within 2.5 mm of native COR. The Iannotti circle should also be independently respected. Although data describing tolerance is not available, it seems prudent to see the prosthetic humeral head lie within 2.5 mm from the circle.
References
- Franta AK, Lenters TR, Mounce D, Neradilek B, Matsen FA 3rd. The complex characteristics of 282 unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg. 2007 Sep-Oct;16(5):555-62. doi: 10.1016/j.jse.2006.11.004. Epub 2007 May 16. PMID: 17509905. ↩︎
- Lawrence TM, Ahmadi S, Sperling JW, Cofield RH. Fixation and durability of a bone-ingrowth component for glenoid bone loss. J Shoulder Elbow Surg. 2012 Dec;21(12):1764-9. doi: 10.1016/j.jse.2011.12.013. Epub 2012 Apr 25. PMID: 22541871. ↩︎
- Youderian AR, Ricchetti ET, Drews M, Iannotti JP. Determination of humeral head size in anatomic shoulder replacement for glenohumeral osteoarthritis. J Shoulder Elbow Surg. 2014 Jul;23(7):955-63. doi: 10.1016/j.jse.2013.09.005. Epub 2013 Dec 8. PMID: 24321169. ↩︎
- Werner, B, Creighton R, Denard P, Lederman E, Romeo A, Griffin J. Prosthetic humeral head center of rotation shift from ideal is associated with inferior clinical outcomes after anatomic total shoulder arthoplasty. J Shoulder Elbow Surg: Seminars in Arthroplasty. 2021 May;31(4):668-676. ↩︎
- Chalmers PN, Granger EK, Orvets ND, Patterson BM, Chamberlain AM, Keener JD, Tashjian RZ. Does prosthetic humeral articular surface positioning associate with outcome after total shoulder arthroplasty? J Shoulder Elbow Surg. 2018 May;27(5):863-870. doi: 10.1016/j.jse.2017.10.038. Epub 2017 Dec 27. PMID: 29289492. ↩︎
Leave a Reply